Spinal cord infarction is caused due to blockage of the major arteries supplying the spinal cord. It's basically a stroke to the spinal cord. Infarctions are most commonly caused by atherosclerosis of spinal arteries. They may also be caused due to aortic atherosclerosis, dissecting aortic aneurysm (chest or back pain with diminished pulses in legs), or hypotension from any cause.
Cardiogenic emboli, vasculitis related to collagen vascular disease like SLE and the antiphospholipid antibody syndrome are other causes
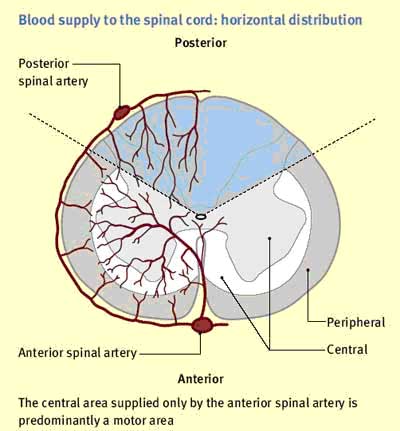
The cord is supplied by three arteries: a single anterior spinal artery and paired posterior spinal arteries.
It shows up abruptly. Onset of symptoms is usually progressive over few minutes to few hours but it may be sudden and dramatic.
Acute infarction in area supplied by anterior spinal artery gives rise to following symptoms:
The most common form is anterior spinal artery syndrome. Infarction in the area supplied by the posterior spinal arteries results in the loss of posterior column functions like loss of position and vibration sense and may not be noticed.
MRI Imaging: Diagnosis is usually done by
MRI. MRI can give a clear picture of compressing space-occupying lesion.
Spinal CT: Spinal CT has only a small role in diagnosis
of spinal infarction.
Myelography: CT myelography
is more sensitive and is used when MRI is not available, contraindicated
or unsatisfactory.
Spinal angiography: Used in cases where spinal arteriovenous
malformations are suspected.
Treatment is symptomatic and supportive. Physical therapy is recommended to help patients recover from paralysis or cope with it. Catheterisation may be required if the patiemt has urinary incontinence.
Prognosis is variable and entirely depends on the severity of damage and how early the treatment has been started. Patients seeking early treatment recover better.
Survival following spinal cord infarction.