Osteoanabolics is a term used to describe a class of medicines used in bone health. It means "bone builders", and it describes the mechanisms of the drugs, not their chemistry or physical properties. Living bone undergoes continuous mineralization and demineralization. When the demineralization rate exceeds the mineralization rate, bone density declines, and many osteoporosis drugs work by lowering the rate of demineralization – or reabsorption of minerals back into the bloodstream.
Most osteoporosis drug therapy is antiresorptive therapy. Bisphosphonates, SERMs, supplemental hormones, and calcitonin are considered antiresorptives. They slow osteoclastogenesis - the resorption of minerals from bone to the bloodstream.
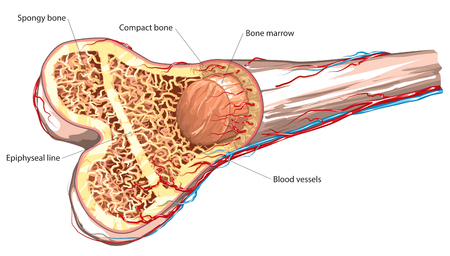
A nice breakdown of the osteoanabolic drugs was presented in a 2012 article in the Indian Journal of Endocrinology and Metabolism. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3354839/ Bone is complex - a composite of inorganic minerals and organic material. By weight bone is about 70% mineral (inorganic), but the organic material - collagen, other proteins, and living cells - are integral to bone. Some osteoanabolic drugs work on inorganic tissue and others work on organic tissue.
Inorganic Tissue Builders include macronutrients calcium and Vitamin D and micronutrients such as magnesium. There is debate about whether supplements of these nutrients should be given to people with no obvious bone problems. See our pages on nutrition and Vitamin D for more on this controversy. But these nutrients do find use in management of osteoporosis.
Recombinant (man-made) parathyroid hormone analogs aren’t exactly the same as parathyroid hormone produced by the body - but they work in the same way. The body makes both parathyroid hormone (PTH, an 84-amino acid chain) and parathyroid hormone related protein (PTHrP, a 34-amino acid chain) They bind to the same receptors in bone tissue. The compounds teriparatide and abaloparatide are hormone analogs approved for treatment of osteoporosis. Teriparatide is the first 34 amino acids of PTH. Abaloparatide is also a 34 amino acid chain; the first 22 are the same as the first 22 amino acids of PTHrP. They help turn preosteoblasts into osteoblasts and thereby increase the growth capacity of the bone. Levels of the enzyme insulin-like growth factor-1 increase, too, and microarchitecture of the bony tissue improves. Parathyroid hormone from cadavers is administered by injection or patch. It is available in some countries, but not the US.
Although expensive and difficult to use (it is administered by injection), teriparatide and abaloparatide work well for a large portion of osteoporosis patients, at least in the first two years of therapy. It has side effects, as do all drugs, but they are generally tolerable for most people. Both teriparatide and abaloparatide increase uric acid in the body so they increase the risk of gout.
Another interesting approach is the administration of calcium receptor antagonists. These stimulate the body to produce more parathyroid hormone. Scientists are interested in this approach, but no drugs are currently on the market. Strontium ranelate is the strontium salt of ranelic acid. Strontium is on the same column of the periodic table as calcium, so it has some similar chemical activity. Some bone cells have calcium-sensing receptors and strontium can act as an agonist on those receptors, thereby promoting the growth of osteoblasts. Strontium ranelate has dual antiresorptive and osteoanabolic effects - it both increases bone formation and reduces bone resorption. However, due to its connection with an increased rate of heart attacks, strontium ranelate is rarely used for osteoporosis treatment.
Drugs acting on the WNT signaling pathway are being investigated, but none are now even close to coming to general availability for patients.
Glucocorticoids are a common cause of secondary osteoporosis, and steroid-induced osteoporosis is due to reduced rates of osteoblastogenesis. It is therefore thought that glucocorticoid-related osteoporosis should be amenable to anabolic agents. A test comparing teriparatide and alendronate in patients found that indeed the osteoanabolic teriparatide provided better results.

Bisphosphonates block bone resorption. They have been widely used for years and although there can be side effects, the medical profession considers them generally safe and effective. More
Selective Estrogen Receptor Modulators (SERMs) are chemical compounds that act on the estrogen receptors in the body. More.
